![]() Primary Dental Evaluation
Primary Dental Evaluation
The dental examination is the conditio sine qua non for arriving at a correct diagnosis and effective dental treatment plan. Every case in which a patient complains of craniofacial pain requires a thorough gathering of information on the status of the teeth, periodontium and mucous membranes, even when there appears to be no connection between the reported complaints and the "typical" toothache. Beware of a superficially conducted "quick diagnosis" which always increases the risk that essential findings and secondary factors will be overlooked, incorrectly evaluated, or forgotten, especially when they seem to bear no apparent relationship to the patient's reported symptoms.
Strictly speaking, the examination begins with the first visual and verbal contact with the patient (physiognomy, skin and facial coloration, posture, gait, speech etc.) Even if not all the information is germane to the dental diagnosis, it is the dentist's duty to identify, to the best of his or her ability, any symptoms that might indicate a systemic illness and to motivate the patient to seek an evaluation from an appropriate specialist (Kirch 1994).
There are various techniques for eliciting and documenting a case history. It is recommended that patients first be allowed to begin describing their history of illnesses in their own words. Because the description of previous illnesses usually proceeds at an irregular pace, after a period of time determined on an individual basis, the caregiver should
politely interrupt the patient's monologue and conduct the consultation further by asking concrete questions concerning the primary and secondary symptoms. Under no circumstances should these questions be leading or suggestive. The diagnosis, treatment plan, and success of the treatment are dependent upon correct interpretation of the findings and therefore upon the knowledge and experience of the clinician. A frequent mistake is the failure to discuss not just the physical, but also psychological conditions as possible etiological factors, especially in cases with ambiguous, indistinctly localized complaints in the face and jaws (Marxkors and Wolowski 1998).
|
Patient history What are your symptoms? |
|
What is your main symptom? |
|
What do you expect from me? |
Special patient-history excerpt from the questionnaire "Manual Functional Diagnosis'*
Primary Dental Evaluation
![]() Findings in the Teeth and Mucous Membrane
Findings in the Teeth and Mucous Membrane
The intraoral evaluation includes in particular:
careful evaluation of the mucous membranes
determination of the status of the teeth,
including detec
tion of caries and periodontal disease
a search for signs of occlusal disturbances
and parafunc-
tion (abrasion, wedge-shaped defects,
enamel cracks and
fractures, and increased tooth mobility)
and
evaluation of the function of fixed and removable partial
dentures and orthodontic appliances.
Numerous diseases, both local and systemic, reveal themselves through changes in the oral mucosa. Therefore the lips, entire vestibule, alveolar ridge, hard and soft palate, tonsils, pillars of the fauces, oropharynx, floor of the mouth, and tongue, including its ventral surface, must be carefully examined for any rashes, discolorations, coatings, or indurations (Veltman 1984). Inflammation localized within the pulp, periodontium, or mucosa can cause pain, varying in degree from light to excruciating, to radiate to the jaws, cheeks, eyes, or ears. The pain can be accompanied secon-
|
|
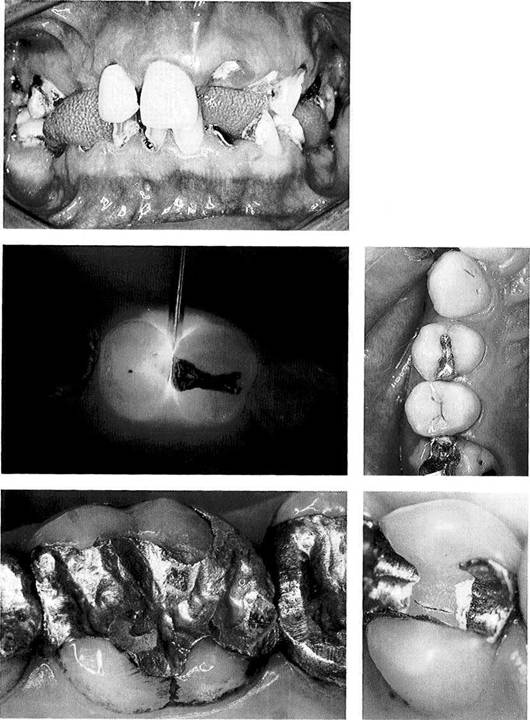
Intraoral inspection
Dentition of a 35-year-old patient exhibiting severe damage from caries and periodontal disease. There is diffuse radiating pain in the right half of the face.
Diagnosis of caries
Transillumination by placing a co!J light probe (by EC Lercher) inter-proximally reveals caries extending into the dentin of the second premolar as evidenced by the increased opacity of the carious toot! structure.
Right: The same region as in the left photograph under regular lighting. The proximal caries on the mesial of the second premolar cannot be seen without the help of a diagnostic aid.
Contributed by K. Pieper
Fractured
filling and
fractured dentin
A functionally inadequate filling with poor marginal integrity is the cause of dentinal pain.
Right: The dentinal fracture on this first premolar was detected only after the occlusal base under the filling was removed. The patient had been experiencing paroxysmal pain in this area upon occlusal loading.
Findings in the Teeth and Mucous Membrane
![]() darily by discomfort in the joints and muscles
and by reduction of lower jaw
mobility. In these cases, treatment is focused upon elimination of the primary cause of the pain. In those cases in which it is difficult to
differentiate among the overlapping
symptoms, selective introduction of local anesthesia as a diagnostic tool can help to identify the source of the pain and the regions to which it radiates.
darily by discomfort in the joints and muscles
and by reduction of lower jaw
mobility. In these cases, treatment is focused upon elimination of the primary cause of the pain. In those cases in which it is difficult to
differentiate among the overlapping
symptoms, selective introduction of local anesthesia as a diagnostic tool can help to identify the source of the pain and the regions to which it radiates.
With mucosal lesions of unknown origin or ulcerations that fail to heal after the presumed cause is removed, a malignant tumor should be suspected. Mistaking an oral carcinoma for a pressure sore from a denture is tragic and inex-
cusable! In case of doubt, a specialist should be consulted. A prolonged course of functional therapy for the masticatory system should be complemented by a repeated dental examination of the mucosa and dentition for the early detection of any new pathology. Normally, during the initial patient evaluation the intraoral examination is supplemented by a radiographic survey (orthopantogram, periapical films).
Caveat: The dentist has an absolute duty to organize and preserve the results of the examination.
|
|
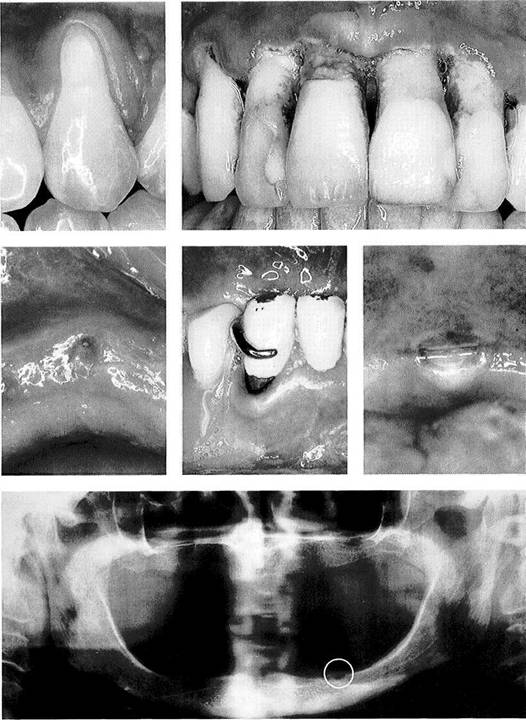
Periodontal findings
Acute necrotizing gingivitis (periodontitis) in a patient with fullblown AIDS.
Left: Pronounced localized gingival recession with severe hypersensitivity at the neck of the tooth.
Traumatic mucosal defects
Left: The same region as shown in the center photograph. The mucosal defect caused a neuralgia-like pain radiating to the right eye.
Center: The mucosal lesion was caused by occlusion of the opposing tooth against the alveolar ridge.
Right: Iatrogenic ulcer in the midline at the transition from hard to soft palate as the result of a posteriorly overextended denture border.
Radiographic findings
This panoramic radiograph shows extensive atrophy of the edentulous mandible with exposure of the left mental foramen (circled). Mechanical irritation of the mental nerve by the lower denture caused pain encompassing the left temporomandibular joint region.
Primary Dental Evaluation
![]() Overview of Dental Examination Techniques
Overview of Dental Examination Techniques
Before beginning the specific functional diagnostic procedure for a patient with pain in the jaws and face or with limited mandibular mobility, all possible intraoral causes for the reported symptoms should be investigated. The goal of conventional dental evaluation is to rule out periodontal and dental structures, as well as intraoral hard and soft tissues, as the source of the pain. The process is similar in principle to manual functional analysis, in that it should be possible to repeatedly initiate or intensify the symptom through probing and/or judicious loading of the tissues. Patient history, extraoral and intraoral inspection (e.g. for
trauma, redness, swelling) and radiographic interpretation (e.g. inflammatory processes) complete the primary dental examination. If there is no significant pathology present that could explain the patient's problem, or if the patient's pain cannot be elicited during the primary dental examination, initial dental treatment procedures are not indicated. Blind action is to be avoided.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]() Overview of dental examination techniques
Overview of dental examination techniques
For patients with acute or chronic jaw and facial pain, a primary dental diagnosis is always performed before the joint-specific examination techniques are carried out.
|
Patient history General medical history Symptoms Chief symptom Primary concern and expectations |
|
|
|
Search for structural lesions |
|
Tooth structure Periodontium Soft tissues Bone structure |
|
Examination for caries |
|
Percussion |
|
|
|
Sensitivity test |
|
|
|
Periodontal status |
|
|
|
Extension of soft tissue |
|
|
|
Tooth position |
|
|
|
Degree of abrasion |
|
|
|
Need for restorations |
|
|
|
Panoramic radiograph |
|
|
|
Mucosal changes |
|